Medical Decision Making (MDM) plays a pivotal role in determining the level of evaluation and management (E/M) services provided. It involves evaluating the complexity of clinical decision-making based on three key elements, only 2 should match.
1. Number and Complexity of Problems Addressed: This considers the severity and quantity of health issues the provider manages during the encounter.
2. Amount and/or Complexity of Data Reviewed and Analyzed: It assesses the extent of data (such as test results, imaging, or patient history) the provider reviews and analyzes.
3. Risk of Complications and/or Morbidity or Mortality of Patient Management: This element evaluates the risk associated with the patient’s condition and the management plan.
MDM is a critical aspect of E/M coding, influencing the choice of codes and reimbursement levels for healthcare services. Understanding and accurately documenting MDM are essential for healthcare providers to ensure proper coding and billing practices.
Introduction to Medical Decision Making
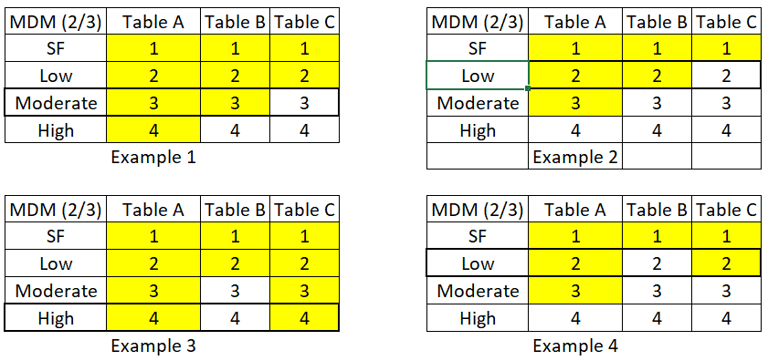
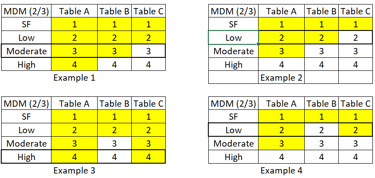
What is mean by 2/3:
MDM has 3 columns, out of which 2 should be matched.
Example 1: - Table A is 4, table B is 3 and Table C is 2, if we see based on 2/3 rule, moderate has 2 highest values matched.
Example 2: Table A is 3, Table B is 2, and Table C is 1 Based on 2/3 MDM rule, low has 2 highest values hence MDM is Low Complexity.
Please solve remaining 2
In E/M coding, the assessment of the number and complexity of problems addressed is important for determining the overall level of Medical Decision Making (MDM). This factor greatly influences the selection of the appropriate E/M code for a patient encounter. Understanding the concept of a "problem" is fundamental in this context.
A problem encompasses any disease, condition, illness, injury, symptom, sign, finding, complaint, or other matter that is addressed at the encounter, regardless of with or without a diagnosis being established at the time of the encounter.
The phrase "with or without a diagnosis being established at that time" indicates that a problem can be considered for MDM complexity selection even if a specific diagnosis has not yet been determined by the healthcare provider during the encounter.
In medical practice, there are instances where a patient presents with symptoms or signs that warrant attention and management, but a definitive diagnosis may require further investigation, testing, or follow-up visits. Despite not having a specific diagnosis at the current encounter, these issues are still considered problems addressed and can be included in the MDM selection process.
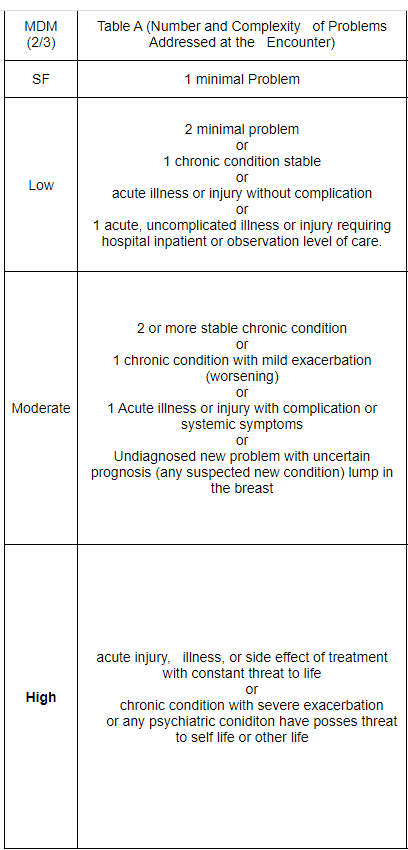
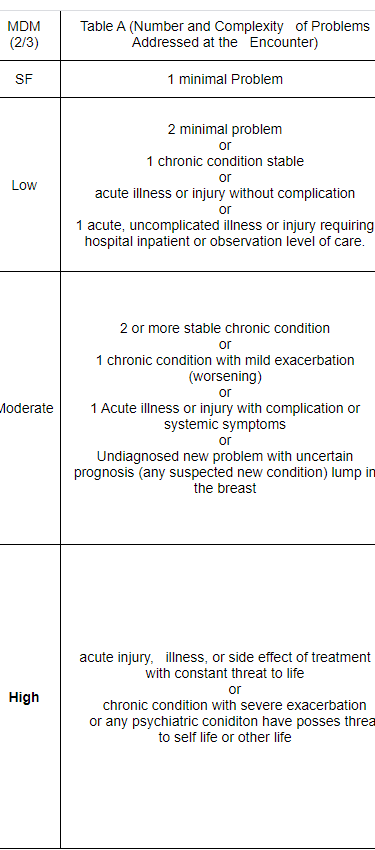
Table A: Number and complexity of problems addressed at the encounter.
A problem is considered addressed when the physician or healthcare professional evaluates or treats it during the encounter. This means that the issue is assessed, and a decision is made on how to manage it, which may include ordering tests or recommending further treatment. Even if the provider decides not to pursue additional testing or treatment due to considerations like the risks involved or the patient's preference, the problem is still considered addressed.
For example, if a patient presents with a persistent cough, the healthcare provider examines the patient, discusses their medical history, and considers whether further tests, such as a chest X-ray or blood tests, are necessary. If the provider decides that the cough is likely due to a common cold and advises rest and fluids without ordering additional tests, the cough is still considered a problem addressed during the encounter.
Not Just Notation: It's not enough for a healthcare provider to just mention in the patient's medical record that another professional is managing a problem. Without additional assessment or care coordination, this notation does not count as the problem being addressed or managed by the provider who is reporting the service.
Imagine a patient with a chronic skin condition is being managed by a dermatologist. During a routine visit to their primary care physician (PCP), the PCP notes in the medical record that the dermatologist is managing the skin condition. However, the PCP does not conduct any further assessment, provide additional treatment, or coordinate care with the dermatologist.
In this scenario, the notation in the medical record that the dermatologist is managing the skin condition does not qualify as the problem being addressed or managed by the PCP. This is because the PCP did not actively evaluate, treat, or coordinate care for the skin condition during the encounter.
Similarly, referring a patient to another healthcare provider without evaluating the problem or considering treatment options does not count as the problem being addressed or managed.
Consider a patient who visits their primary care physician (PCP) with symptoms of a persistent cough. Instead of conducting a thorough evaluation, such as taking a detailed medical history, performing a physical examination, and ordering relevant tests (e.g., chest X-ray, blood tests), the PCP immediately refers the patient to a pulmonologist without considering other possible causes or treatment options.
In this scenario, the referral made by the PCP would be considered a non-qualifying referral. This is because the PCP did not conduct a proper evaluation to determine the underlying cause of the cough or consider alternative treatment options before referring the patient to the pulmonologist. As a result, the referral does not meet the criteria for addressing or managing the patient's problem.
Hospital Inpatient and Observation Care Services: Understanding Problem Addressed: For hospital inpatient and observation care services, the problem addressed is the problem status on the date of the encounter, which may be significantly different from the status on admission. It is the problem being managed or co-managed by the reporting physician or other qualified healthcare professional and may not be the cause of admission or continued stay.
In the context of hospital inpatient and observation care services, it's important to recognize how the problem addressed is determined. Unlike other settings, the problem addressed in these settings is the problem status on the date of the encounter, which can vary significantly from the status on admission. This distinction is crucial for accurately documenting and coding the care provided.
Example Scenario:
Imagine a patient is admitted to the hospital for chest pain. Upon admission, the patient undergoes various tests and evaluations, and it is determined that the chest pain is due to a non-cardiac cause, such as musculoskeletal pain. However, during the hospital stay, the patient develops pneumonia, which becomes the primary focus of care.
In this scenario, the problem addressed for the hospital inpatient or observation care services would be the pneumonia, as it is the problem being managed or co-managed by the reporting physician or other qualified healthcare professional during the encounter. Even though the chest pain was the reason for admission, it may not be the primary focus of care during the hospital stay, and therefore, it may not be the problem addressed for coding purposes.
Minimal Problem: A minimal problem refers to a situation where the service provided does not necessarily require the direct presence of the physician or other qualified healthcare professional. However, the service is performed under their supervision. This concept is applicable to specific CPT codes such as 99211 and 99281, which represent services that are minimal in nature and typically do not involve complex medical decision-making or significant physician involvement.
Examples:
Suture Removal: Patients who require suture removal following a minor procedure can receive this service under minimal problem coding. The healthcare provider can oversee the removal process without needing to assess complex medical issues.
Blood Pressure Checks: Routine blood pressure checks for monitoring purposes are another example of a minimal problem service. These visits are straightforward and primarily involve measurement and documentation under supervision.
PPD reading: Administering and interpreting a tuberculin skin test.
Self-limited or minor problem: A problem that runs a definite and prescribed course, is transient in nature, and is not likely to permanently alter health status.
A patient presents with symptoms such as a runny nose, sore throat, and cough, typical of a viral URI. The condition is self-limited, meaning it will resolve on its own without specific medical treatment, and it is not likely to permanently alter the patient's health status.
A healthcare provider may provide minimal intervention, such as advising the patient to rest, stay hydrated, and possibly recommending over-the-counter remedies for symptom relief. This encounter would be straightforward and would not involve significant medical decision-making or complex management, aligning with the definition of a self-limited or minor problem.
Stable, chronic illness:
Chronic illness is a health problem that lasts for at least a year or until the patient dies. It doesn't matter if the condition's stage or severity changes over time—it's still considered chronic.
The term "stable" depends on the patient's treatment goals. If a patient hasn't reached their treatment goal, even if their condition hasn't changed and they're not in immediate danger, they're not considered stable. For example, if someone has consistently high blood pressure and the goal is to lower it, they're not stable—even if their blood pressure isn't changing and patient is asymptomatic. Without intervention, there is a notable risk of morbidity.
To elaborate further, in medical decision-making, the term "stable" depends on the patient's treatment goals. A patient is deemed stable only if they have achieved their treatment goal. Even if a patient's condition has not worsened and there is no immediate threat to their life or function, if the treatment goal has not been met, the patient is not considered stable.
Example: Consider a patient with diabetes whose treatment goal is to maintain blood sugar levels within a specific range. If the patient's blood sugar levels remain persistently high despite treatment, they are not considered stable, even if they are asymptomatic and there is no immediate threat to their health. In this case, the risk of morbidity without treatment remains significant, highlighting the importance of ongoing management and monitoring.
For instance, consider a patient with persistently poorly controlled blood pressure. If the goal of treatment is to achieve better control, the patient is not considered stable even if their blood pressure readings are not changing and they are not experiencing any symptoms. This is because the patient has not reached the treatment goal of better control, and without treatment, there is a significant risk of morbidity.
Acute, uncomplicated illness or injury:
Acute, uncomplicated illness or injury typically presents as a recent or new short-term problem with a low risk of serious health complications when treated. The expected outcome is full recovery without any lasting functional impairment.
In cases of acute, uncomplicated illness or injury, there is generally little to no risk of mortality with appropriate treatment. These types of issues are often self-limited or minor, meaning they are expected to resolve on their own or with minimal medical intervention.
However, if a problem persists and does not resolve as expected, despite following a definite and prescribed course of treatment, it may be classified as an acute, uncomplicated illness.
Stable acute illness:
This describes a category of low-level conditions that require inpatient or observation care and may apply to a patient that has been stabilized in a hospital or nursing facility but is still receiving treatment.